1) "55 year old male patient came with the complaints of
Chest pain since 3 days
Abdominal distension since 3 days
Abdominal pain since 3 days and decreased urine output since 3days and not passed stools since 3days
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
A. ANATOMICAL LOCATIONS WITH ETIOLOGY:
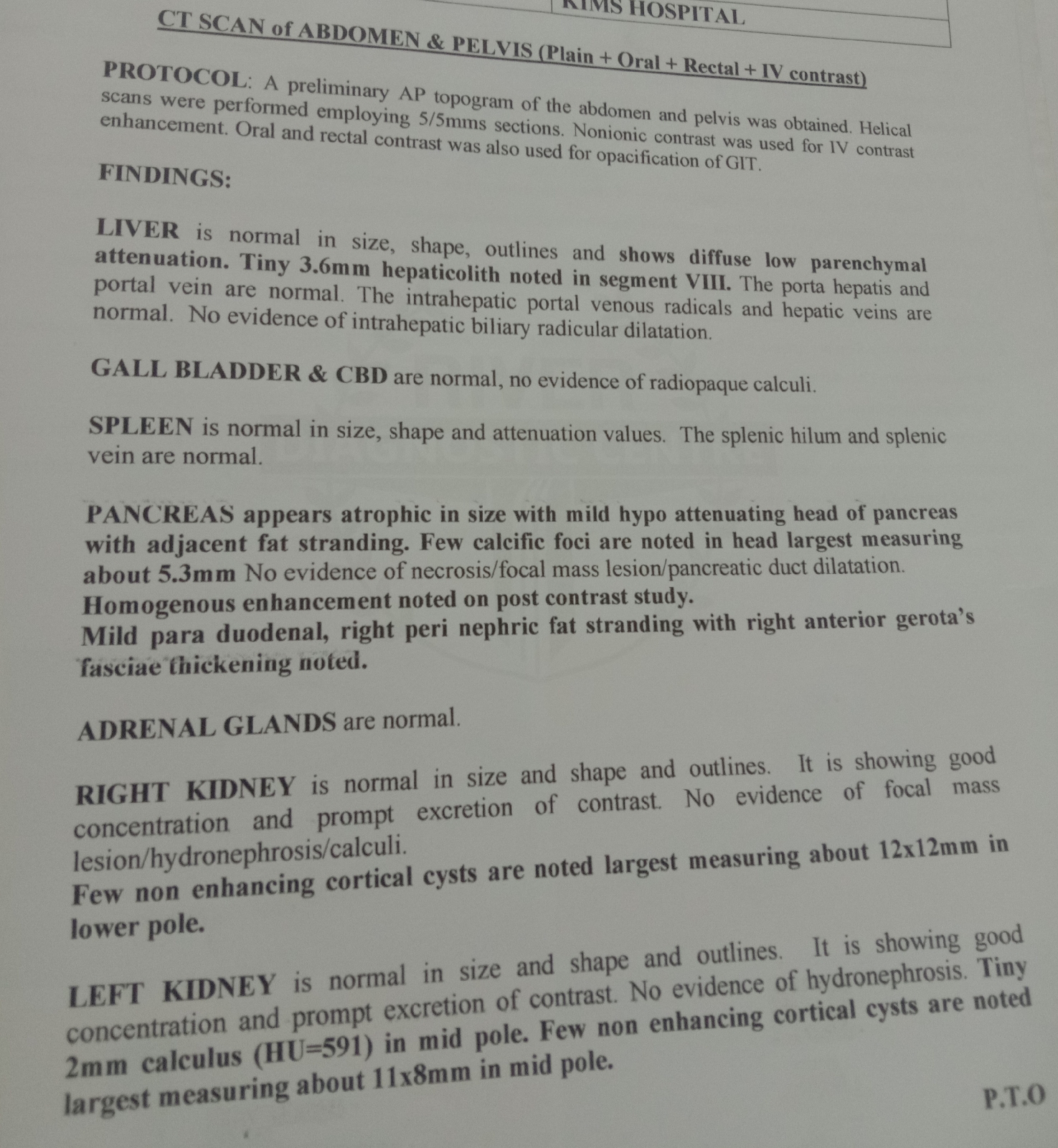
GIT (Pain abdomen) :
Etiology: Pancreatitis secondary to ? chronic alcoholism
KIDNEYS (Oliguria) :
Etiology: AKI (pre renal due to fluid loss in. pancreatitis)
Sepsis induced ATN
HEART / LUNGS (SOB) :
Etiology: AKI leading to fluid overload and heart failure.
Pancreatitis leading to pleural effusion / ?ARDS
GIT (Constipation) :
Etiology: ? paralytic ileus secondary to pancreatitis
SEQUENCE OF EVENTS:
Congenital bow leg deformity
Alcohol & smoking (30 years)
Abdominal pain & distention , SOB , chest pain , decreased urine output (3 days)
OUTCOMES:
Urine output increased , pedal edema and SOB decreased (Day-2)
Altered sensorium (Day-3)
Dialysis done (Day-4)
Bilious vomiting (Day-5)
Dialysis done (Day-6)
Abdominal pain & vomitings subsided (Day-8)
Now the patient is on hemodialysis for his renal failure
b) What are the pharmacological and non pharmacological interventions used in the management of this patient and what are the efficacy of each one of them?
A. PHARMACOLOGIC :
https://link.springer.com/article/10.1007/s00534-005-1050-8
1. Fluid replacement :
Increased vascular permeability in acute pancreatitis causes the loss of intravenous fluid and reduces plasma volume. In severe cases, in patients with massive ascites, pleural effusion, and retroperitoneal and mesenteric edema, circulating plasma volume decreases markedly. Hypovolemia may lead to shock and acute renal failure, and, because hypovolemic shock may impair the pancreatic microcirculation and promote pancreatic ischemia and necrosis, restoration and maintenance of plasma volume is crucial in severe acute pancreatitis.
2. Antibiotics : No role of antibiotics
3.Tramadol : For pain management
4. Zofer : For vomitings
5. Pantop : To prevent gastritis and further damage to pancreas by inhibiting gastrin
6. Lasix: For fluid overload
7.Nebulization: For wheezing and crepts
B. NON - PHARMACOLOGICAL
1)nill per mouth
https://pubmed.ncbi.nlm.nih.gov/27107634/
2)ryles tube catheterisation
3)oxygenation
2)A 55 year old male, shepherd by occupation, presented to the OPD with the chief complaints of fever (on and off), loss of appetite, headache, body pains, generalized weakness since 2 months, cough since 2 weeks and vomitings and pain abdomen since 2 days.
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
A. ANATOMICAL LOCATIONS WITH ETIOLOGY:
BONE MARROW
Etiology: Multiple myeloma
KIDNEYS
Etiology: AKI due to multiple myeloma
HEMATOLOGICAL (ANEMIA)
Etiology: secondary to multiple myeloma
LUNGS
Etiology: Tuberculosis (Increased susceptibility to infections)
TIMELINE OF EVENTS:
Alcohol & smoking (35 years)
Stopped alcohol (4 years)
Fever , generalised weakness & anemia - 2 units blood transfusion (1.5 years)
Stopped smoking (4 months)
Low grade fever , generalized weakness , headache , neck pain , loss of appetite , weight loss (2 months)
Cough & SOB (2 weeks)
Vomiting & pain abdomen (2 days)
OUTCOME:
Some symptomatic relief and referred to higher centre in need for oncologist
b) What are the pharmacological and non pharmacological interventions used in the management of this patient and what are the efficacy of each one of them?
A. PHARMACOLOGICAL:
1. Antibiotics
2. Blood transfusion
B. NON - PHARMACOLOGICAL
Pleural fluid analysis
3) 51 Year old man with complaints of B/L pitting pedal edema from 5 to 6months,abdominal distension from 2 to 3 days,SOB from 3days.
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
A. ANATOMICAL LOCATIONS WITH ETIOLOGY:
HEART (HFrEF - pedal edema , abdominal distention and SOB) :
Etiology: Microvascular dysfunction DM and HTN
CNS (Seizures) :
SEQUENCE OF EVENTS:
Tobacco chewing (40 years)
Alcohol (10 years)
DM (7 years)
HTN (5 years)
1st Episode GTCS (3 years) & AF with HFpEF
2nd Episode GTCS (2 years)
HFrEF & Anasarca (1 year) - (subsided with medication)
Pedal edema (6 months)
Increased pedal edema , abdominal distention , SOB and decreased urine output (3 days)
CURRENT OUTCOME:
Symptomatically releived and discharged
b) What are the pharmacological and non pharmacological interventions used in the management of this patient and what are the efficacy of each one of them?
A) Pharmacological interventions
https://heart.bmj.com/content/104/5/407(meta analysis with each class of drugs)
Preload reducers.
Diuretics.
Afterload reducers-ace inhibitors.
Rate controlling agents-beta blockers.
Antiepileptics for known case of epilepsy.
Insulin for glycemic control in diabetes.
B) Non pharmacological interventions
Salt and fluid restriction
https://pubmed.ncbi.nlm.nih.gov/23787719/
Individualized salt and fluid restriction can improve signs and symptoms of CHF with no negative effects on thirst, appetite, or QoL in patients with moderate to severe CHF and previous signs of fluid retention.
4) 31 yr old man with B/L pedal edema with scrotal and penile swelling since 2 months
https://nairaditya97.blogspot.com/2020/11/31-yr-old-male-with-bl-pedal-edema-with.html?m=1
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
A. ANATOMICAL LOCATIONS WITH ETIOLOGY:
HEART FAILURE (pedal edema , penile & scrotal swelling and SOB) :
Etiology: Alcohol causing wet beriberi
AXONAL SENSORY POLYNEUROPATHY:
Etiology: Alcohol
Other conditions causing beri beri are:
. Genetic beri beri
. pregnancy
. hyperthyroidism
. chronic liver disease
. kidney dialysis
. large bout of diarrhea
EVENTS TIME LINE:
Alcohol & khaini (3 years)
Pins and needles (1 year)
Palpitations (8 months)
PND (3 months)
Pedal edema and SOB (2 months)
CURRENT OUTCOME:
Completly relieved of his symptoms as the wet beriberi resolved.
b) What are the pharmacological and non pharmacological interventions used in the management of this patient and what are the efficacy of each one of them?
A. PHARMACOLOGICAL
1. Lasix
https://www.ncbi.nlm.nih.gov/books/NBK69174/
2. Thiamine
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3865826/#:~:text=Compared%20with%20placebo%20(2%20trials,0.64%25%2C%205.93%25).
3. Telmisartan: For afterload reduction in heart failure.
B. NON - PHARMACOLOGICAL
1. Salt and fluiPHARMACOLOGICAL
https://pubmed.ncbi.nlm.nih.gov/23787719/